Things not to miss - Aortic Dissection
Elderly man presented to medical casualty with severe central chest pain. He was restless and was sweating. Blood pressure was 180/100 and pulse rate was 96/min. There was a murmur. Lungs were clear. Urgent ECG was taken.
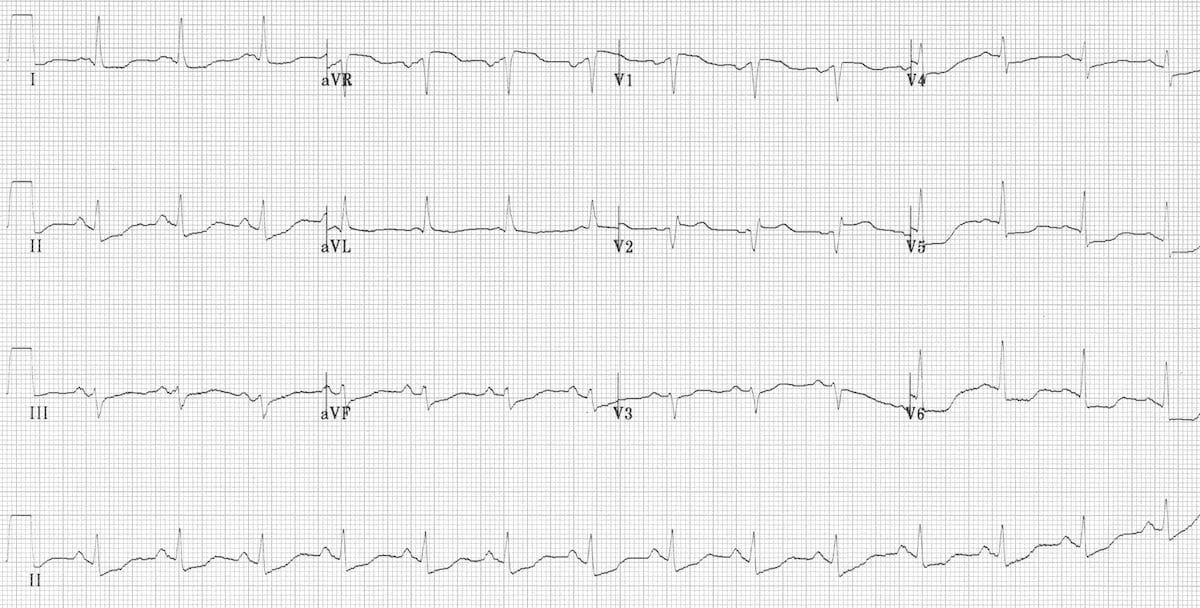

As there were widepread ST depressions the house officer started the patient on aspirin, clopidogrel, atorvastatin and enoxaparin. For pain he prescribed GTN and morphine which calmed down the patient.
Two hours later patient again complained of severe chest pain which did not respond to GTN. The registrar was summoned. Blood pressure was still 180/100 and the heart rate was 120/min. Registrar noted also noted a murmur. The differential diagnosis of aortic dissection was immediately considered. There was a radio femoral delay!
After urgent management a CT aortogram was done which showed a massive dissection of aorta extending from aortic root down to aortic bifurcation. The had a cardiac arrest a few hours later.
Lesson.
~ Any chest pain could be an aortic dissection. Consider that before prescribing anticoagulation/ thrombolytic.
~ Clinical features of aortic dissection include
- Pain radiating from back
- Radio femoral/ radio radial delay or a pulse deficit
- A murmur - particularly that of an aortic regurgitation
~ Remember - ANY MURMUR CAN BE A NEW MURMUR!
~ Take a seniors opinion if theres even a slightest suspicion of a dissection.
~ 2D echo/ USS/ Chest Xray all can be helpful for the diagnosis. CT aortogram is the investigation of choice.
Chest Xray showing a wide mediastinum.
~ Acute management includes maintating systolic blood pressure around 120-100mmHg and maintaining a pulse rate below 60/min. The drugs of choice are beta blockers. Eg. Labetolol, Esmolol.
ECG was taken from the page Life in the Fast Lane. Xray was from the medscape.


Comments
Post a Comment